

Return to Index Next Lesson Return to: Basic First Aid or Field Manuals
After completing this lesson, you should be able to:
1-1. Identify procedures for tactically managing a casualty under combat conditions.
1-2. Identify the major causes of battlefield deaths.
1-3. Identify the three phases of tactical combat casualty care.
1-4, Identify care provided in each phase of tactical combat casualty care.
REFERENCES
STP 21-1-SMCT, Soldier's Manual of Common Tasks: Skill
Level 1.
FM 4-25.11, First Aid.
Training Support Package 071-D-2321 / First Aid 6 (Perform Tactical Combat
Casualty Care).
LESSON 1
PERFORMING TACTICAL COMBAT CASUALTY CARE
1-1. BATTLEFIELD DEATHS
a. Most combat deaths occur on
the battlefield before the casualties reach a MTF. Most of these deaths are
inevitable (massive trauma, massive head injuries, and so forth). However,
some conditions such as bleeding from a wound on an extremity (arm or leg),
tension pneumothorax, and airway problems can be treated on the battlefield.
This treatment can be the difference between a combat death on the
battlefield and a recovering soldier in a MTF. It has been estimated that
proper use of self-aid and buddy-aid skills can reduce battlefield deaths by
up to 15 percent (mostly from methods to control bleeding from the
extremities). Table 1-1 gives an estimated breakdown of battlefield deaths.
b. In combat, the combat medic
may not be able to reach the casualty in time to save the casualty's life,
especially if the casualty is losing a great deal of blood quickly. The
combat medic may even become a casualty and require aid himself. In such a
situation, quick self-aid (the injured soldier treating himself) or
buddy-aid (the injured soldier being treated by a fellow soldier) is needed.
For example, over 2500 soldiers died in Viet Nam caused by hemorrhage from
extremity wounds even though the soldiers had no other serious injuries.
Proper application of pressure dressings and tourniquets by fellow soldiers
could have saved most of these casualties.
DEATHS CAUSED BY GROUND COMBAT
31%--Penetrating head trauma
25%--Surgically uncorrectable torso trauma
10%--Potentially correctable surgical trauma
9%--Exsanguination (bleeding) from extremity wounds
7%--Mutilating blast trauma
5%--Tension pneumothorax
1%--Airway problems
12%--Died of Wounds after being evacuated to a medical
treatment facility (usually from infections and complications of shock)Table 1-1. Estimated breakdown of battlefield deaths.
1-2. TACTICAL COMBAT CASUALTY CARE
Tactical combat casualty care (TCCC) can be divided into
three phases. The first is care under fire; the second is tactical field
care; the third is combat casualty evacuation care.
a. Care
Under Fire. In a situation in which the casualty and you are under
hostile fire, you are very limited as to the care you can provide. Paragraph
1-3 discusses this situation.
b. Tactical
Field Care. In tactical field care, you and the casualty are in a
protected or safe environment. In this situation, you are free to provide
casualty care to the best of your ability. Paragraph 1-4 discusses this
situation.
c. Combat
Casualty Evacuation Care. In the third situation, care is being given to
the casualty during casualty evacuation (CASEVAC). Casualty evacuation
refers to the care given to the casualty while the casualty is awaiting
pickup or is being transported by a nonmedical vehicle, such as a vehicle
used to transport troops or supplies. Paragraph 1-5 discusses this
situation.
NOTE:
Casualty evacuation is different from medical evacuation (MEDEVAC). In
MEDEVAC, a designated medical vehicle (ground ambulance or air ambulance) is
used.
1-3. PERFORMING CARE UNDER FIRE
Care under fire is rendered at the scene of the injury
while you and the casualty are still under effective hostile fire. In such a
situation, you should perform the following actions.
a. Return fire as directed or required before providing medical treatment.
b. Determine if casualty is alive or dead.
c. Provide tactical care to the live casualty. Reducing or eliminating enemy fire may be more important to the casualty's survival than the treatment you can provide.(1) Suppress enemy fire.d. If you can safely move the casualty to safety, do so. Administer only life-saving hemorrhage control while still under enemy fire.
(2) Use cover or concealment (smoke) to conceal the casualty, if possible.
(3) If the casualty is able, direct him to return fire, move to cover, and administer self-aid (control bleeding). If the casualty is unable to move and you are unable to move the casualty to cover, have casualty "play dead."(4) Keep the casualty from sustaining additional wounds.
(5) Reassure the casualty.
NOTE: Hemorrhage refers to serious bleeding.
(1) If the casualty has severe bleeding from a limb or has suffered amputation of a limb, quickly apply a tourniquet before moving the casualty to safety. Do not take time to check the casualty for breathing or airway obstruction.
(2) Move the casualty, his weapon, and any mission-essential equipment to cover as the tactical situation permits. Do not take the time to move equipment that is not mission essential.
NOTE: You must determine the relative threat of the tactical situation versus the risk to the casualty. Can you remove the casualty to a place of relative safety without becoming a casualty yourself? Is the casualty safer where he is? If possible, seek guidance and assistance from your leader.
e. Recheck the bleeding control measures as the tactical situation permits.
1-4. PERFORMING TACTICAL FIELD CARE
Perform tactical field care when you and the casualty are
no longer under direct enemy fire.
NOTE:
Tactical field care also applies to situations in which an injury has
occurred on a mission when there is no hostile fire. Available medical
supplies are limited to those carried into the field by individual soldiers.
a.
Communication. Communicate the medical situation to the unit leader.
Ensure that the tactical situation allows time to treat the casualty before
initiating treatment procedures. Inform the unit leader if:
(1) The casualty will not be able to continue his mission.
(2) There is any significant change in casualty's status.
b. General
Impression. Form a general impression of the casualty as you approach
(extent of injuries, chance of survival, and so forth). Continue to evaluate
the tactical situation for possible danger to yourself and the casualty.
NOTE: If the
casualty has suffered from a blast or penetrating trauma and has no signs of
life (no pulse, no respirations), do not perform cardiopulmonary
resuscitation (CPR). These casualties will probably not survive and you may
expose yourself to enemy fire.
c. Level of
Consciousness. When possible, determine the casualty's level of
consciousness using the AVPU system. Ask questions that require more than a
"yes" or "no" answer, such as, "What is your name? What is the date? Where
are we?" Recheck the casualty's level of consciousness about every 15
minutes to determine if the casualty's condition has changed. Report your
findings to the combat medic or combat lifesaver when he comes.
(1) A--The casualty is alert, knows who he is, the date, where he is, etc.
(2) V--The casualty is not alert, but does responds to verbal commands.
(3) P--The casualty responds to pain, but not verbal commands.
(4) U--The casualty is unresponsive.
NOTE:
Maintaining a check on the casualty's level of consciousness is especially
important when the casualty has suffered a head injury.
NOTE:
If the casualty is alert or responds to voice, do not check the casualty's
response to pain.
NOTE: To
check a casualty’s response to pain, rub his breastbone briskly with a
knuckle or squeeze his first.
d. Airway.
Assess and secure the casualty's airway.
(1) If the casualty is conscious, able to speak, and is not in respiratory distress, no airway intervention is needed.
(2) If the casualty is unconscious, perform the following.(a) Use a head-tilt/chin-lift or jaw thrust to open the airway. The head-tilt/chin-lift is the normal method of opening the casualty's airway. The jaw thrust is used if you suspect the casualty has suffered injury to the head, jaw, or spine (back).
NOTE: The muscles of an unconscious casualty's tongue may have relaxed, causing his tongue to slide to the back of his mouth and cover the opening to his trachea (windpipe). Using the head-tilt/chin-lift or jaw thrust removes the blockage by moving the tongue away from the trachea. Moving the tongue away from the opening to the trachea may result in the casualty breathing on his own again without the need for rescue breathing techniques.
(b) Check the casualty for breathing. Place your ear over the casualty's mouth and nose with your face toward the casualty's chest while maintaining the casualty's airway (head-tilt/chin-lift or jaw-thrust). Look for the rise and fall of the casualty's chest and abdomen. Listen for sounds of breathing. Feel for his breath on the side of your face.1) If the casualty is not breathing, begin rescue breathing.
2) If the casualty is breathing on his own, insert a nasopharyngeal airway (NPA) to maintain the airway.
NOTE:
Procedures for opening the airway, performing rescue breathing, and
inserting a nasopharyngeal airway are described in Lesson 3 of this
subcourse.
e. Chest.
Assess and treat the casualty for chest injuries (Lesson 4).
(1) Expose the chest and check for equal rise and fall. Remove the minimum of clothing required to expose and treat injuries. Protect the casualty from the environment (heat and cold) as much as possible.
(2) Examine the chest for wounds. Check for both entrance and exit wounds (sucking chest wounds). (3) Immediately seal any penetrating injuries to the chest with an occlusive dressing. Sealing the wound keeps air from entering the wound. If air can freely enter through the wound, the casualty's affected lung will collapse.
(4) Monitor the casualty for progressive severe respiratory distress (breathing becomes more labored and faster). If respiration becomes progressively worse, consider this a tension pneumothorax and decompress the affected chest side with a 14-gauge needle inserted at second intercostal space (ICS) at midclavicular line (MCL). Secure the catheter in place.
CAUTION:
Only perform needle chest decompression on a
casualty with a penetrating (sucking) chest wound.
f. Bleeding.
Identify and control major bleeding (see Lesson 5).
(1) Apply a tourniquet to a major amputation of the extremity. (2) Apply an emergency bandage and direct pressure to a severely bleeding wound.(a) If conventional methods of controlling severe bleeding (emergency bandage, direct pressure, pressure dressing, hemostatic dressing, and so forth) do not control the bleeding on an extremity, apply a tourniquet.
(b) If a tourniquet was previously applied, consider changing the tourniquet to an emergency bandage or pressure dressing to control bleeding. Leave the tourniquet in place while doing this. Loosen it, but do not remove it. If conventional methods are not able to control hemorrhage, retighten the tourniquet until bleeding stops.
NOTE: By converting
the tourniquet to a pressure dressing or controlling the bleeding by other
methods, you may be able to save the limb of the casualty if the tourniquet
has not been in place for 6 hours. If tourniquet has been in place for more
than 6 hours do not remove the tourniquet.
g. Other Wounds. Identify and
treat other wounds. Dress all wounds, including exit wounds. Remember to
remove only the minimum of clothing required to expose and treat injuries.
Protect the casualty against the environment (hot and cold temperatures, and
so forth).
h. Fractures. Splint any obvious
long bone fractures (see Lesson 6).
i. Combat Pill Pack. Administer
pain medications and antibiotics (combat pill pack) to any soldier wounded
in combat. Do not administer your own pack since you may need them yourself
and you have no extra combat pill packs in your aid bag.
NOTE: Each
soldier will be issued a combat pill pack prior to deployment on tactical
missions.
j. Positioning the Casualty.
(1) Usually, you will roll the casualty onto his side and position the casualty's arms and legs to stabilize him in the recovery position (figure 1-1). This position allows accumulated blood and mucus to drain from the casualty's mouth instead of choking the casualty. This is especially important if the casualty is unconscious and you cannot stay with him.
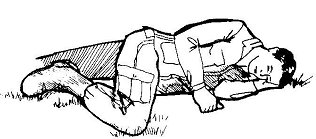
Figure 1-1. Unconscious casualty placed in the recovery position.
(a) If the casualty has an open chest wound without a needle chest decompression, position the casualty with the injured side toward the ground. The body pressure acts to "splint" the affected side.(2) For some injuries, the recovery position is not used. For example, a soldier with an abdominal wound is positioned on his back with his knees flexed (knees raised with the bottoms of his feet on the ground). If the casualty is being treated for shock (severe blood loss, and so forth), the casualty is placed on his back with his feet elevated (placed on a log, pack, or other stable object).
(b) If a needle chest decompression has been performed, position the casualty with the uninjured side toward the ground.
1-5. PERFORMING COMBAT CASUALTY EVACUATION CARE
Prepare the casualty for evacuation, if needed.
a. When possible, the casualty is transported by medical ambulance (helicopter or ground ambulance) to a medical treatment facility (MTF). If a medical ambulance is used to transport a casualty, it is called medical evacuation (MEDEVAC).
b. If a ground or air ambulance is not available, the casualty may be transported by nonmedical means. For example, a truck used to haul troops or supplies may be used to transport casualties to a medical treatment facility. When nonmedical vehicles are used to transport a casualty, it is called casualty evacuation (CASEVAC).
c. Sometimes a casualty must be moved to another area where he can be placed on a vehicle, either MEDEVAC or CASEVAC. If the casualty needs to be carried, he should be moved on a litter. Lesson 7 describes how to prepare and use the SKED® litter and how to make improvised litters.
LESSON EXERCISES: LESSON 1
INSTRUCTIONS: Answer the
following exercises by marking the letter of the response that best
answers the question or best completes the sentence or by writing the
answer in the space provided.
After you have answered all of the exercises, check your
answers against the "Solutions to Lesson Exercises" at the end of the
exercises. For each exercise answered incorrectly, reread the lesson
material referenced.
1. Of the deaths that occur during ground combat, about what percent die before reaching a medical treatment facility?
a. 10 percent.
b. 20 percent.
c. 50 percent.
d. 90 percent.
2. Your unit is in ground combat. You see a soldier fall as though he has been shot. Your primary duty is to:
a. Continue firing at the enemy.
b. Stop firing and go to the fallen soldier.
3. Of the following types of deaths occurring during ground combat and before reaching a medical treatment facility, select the type of preventable death from which more soldiers died.
a. Tension pneumothorax.
b. Blocked airway.
c. Bleeding from wounds to the extremities.
d. Heart attack.
4. What is the only aid rendered while under fire?
a. Perform cardiopulmonary resuscitation.
b. Control bleeding with a tourniquet.
c. Relieve tension pneumothorax.
d. Control pain and infection.
5. You and a casualty are under fire. The casualty is
conscious and able to fire his weapon. What should you tell him to do?_____________________________________________________________
6. You and a casualty are under fire. The casualty has
a severe wound to the arm. You can administer treatment without endangering
the mission. What treatment should you administer?_____________________________________________________________
7. You have been wounded and are still under enemy
fire. You are unable to return fire and there is no safe cover nearby. What
should you do?_____________________________________________________________
8. You can move a casualty out of enemy fire. Should
you try to retrieve his weapon also?
a. Yes, if the tactical situation permits.
b. Yes, under all circumstances.
c. No.
9. A nasopharyngeal air is inserted to maintain the casualty's airway as part of:
a. Care under fire.
b. Tactical field care.
c. Both care under fire and tactical field care.
10. What is in the combat pill pack that you and other
soldiers carry in combat?___________________________________________________________
11. Why must a penetrating chest wound be sealed?
a. To keep air from entering through the wound.
b. To keep air from escaping through the wound.
c. To control bleeding.
12. You are going to administer a combat pill pack to a casualty. You should administer:
a. The casualty's pack.
b. Your personal pack.
13. Classify the following casualties according to the
AVPU system.
____ Casualty number one moves his arm when you tell him
forcefully to do so and responds to pain when you moved him , but does not
respond otherwise.
____ Casualty number two does not appear to have any
injuries other than a bruise on the side of his head; however, he does not
respond to anything you do.
____ Casualty number three has been shot in the leg and is
yelling at you to "Hurry and do something."
____ Casualty number four groans when you try to move his
injured leg, but does not respond when you ask him how he feels or tell him
to move his uninjured arm.
14. What is the most likely cause of a blocked airway
in an unconscious casualty?_______________________________________________________________________________________
____ Apply a pressure dressing to a serious wound on the casualty's arm.
____ Check the casualty for breathing using Look, Listen, and Feel.
____ Open the casualty's airway using the head-tilt/chin-lift.
____ Splint the casualty's fractured leg.
____ Apply a seal to an open chest wound.
17. You must leave an unconscious casualty to perform other duties. How should you normally position the casualty before you leave?
a. On his back.
b. On his side.
c. On his chest.
d. In whatever position you originally found him.
18. Why did you position the casualty
in exercise 17 in the manner you chose?_______________________________________________________________
19. A casualty is to be evacuated to a military medical
treatment facility. If the casualty is transported using a medical ground or
air ambulance, it is called a ______________________.
If a truck normally
used to carry supplies to troops in the field is used to transport the
casualty, it is called a _____________________________________________ .
SOLUTIONS TO LESSON EXERCISES: LESSON 1 (scroll down)
1. d (para 1-1a,Table 1-1)
2. a (para 1-3)
3. c (Table 1-1)
4. b (paras 1-3d, d(1))
5. Return fire (para 1-3c(3))
6. Tourniquet (para 1-3d(1))
7. Play dead (para 1-3c(3))
8. a (para 1-3d(2))
9. b (para 1-4d(2)(b)2)
10. Pain medication and antibiotics (para 1-4i)
11. a (para 1-4e(3))
12. a (para 1-4i)
13. Casualty number one: V
Casualty number two. U
Casualty number three. A
Casualty number four P (para 1-4c)
14. Casualty's tongue relaxes, slides to the back of the mouth and covers
the opening to the trachea (para 1-4d(2) NOTE).
15 Head-tilt/chin-lift Jaw thrust (para 1-4d(2)(a)
16. __4__ Apply a pressure dressing to a serious wound on the
casualty's arm.
__2__ Check the casualty for breathing using Look, Listen, and
Feel.
__1__ Open the casualty's airway using the head-tile/chin-lift.
__5___ Splint the casualty's fractured leg.
__3__ Apply a seal to an open chest wound. (paras 1-4d, e, f, h)
17. b (para 1-4j(1), fig 1-1).
18. This position allows accumulated blood and mucus to drain from the
casualty's mouth (para 1-4j(1))
19. Medical evacuation (MEDEVAC) (para 1-5a) Casualty evacuation
(CASEVAC) (para 1-5b)
Please Read The Website Disclaimer!
Copyright 1986-2012, The Survival & Self-Reliance Studies Institute (SSRsi), All
Rights Reserved
Site conceptualized, designed, created & maintained by MEG Raven
Snail Mail: SSRsi, PO Box 2572 Dillon, CO. 80435-2572